

Late-Life Depression and
Response to Antidepressants
Late-life depression (LLD), defined as depression in adults over the age 60, may be a biologically-distinct disorder compared to depression in younger adults. LLD is challenging to treat due to the changes that occurs with aging, therefore we are trying to understand how genetic variation affects response to antidepressants in late life.
We reviewed the scientific literature to provide a summary of the literature exploring genetic associations with antidepressant treatment outcomes in late-life.

Our Conclusion:
The most substantial amount of evidence exists for the CYP2D6 metabolizer status, SLC6A4 5-HTTLPR, and BDNF rs6265.
These findings are consistent in the literature when not restricting to older adults, suggesting that similar treatment recommendations may be provided for older adults regarding genetic variation, such as those outlined for CYP2D6 by the Clinical Pharmacogenetics Implementation Consortium. Nonetheless, further studies are required in well-characterized samples, including genome-wide data, to validate if similar treatment adjustments are appropriate in older adults, given that there appear to be significant effects of genetic variation on antidepressant treatment factors.
Did you know?
Up to 15% of older adults over the age of 60 living in the community may present with symptoms of depression.
Candidate and Genome-Wide Studies
A Candidate-Gene Approach
The primary objective of this study was to investigate five putatively functional variants of the norepinephrine transporter (SLC6A2, NET) and serotonin transporter (SLC6A4, SERT) genes and remission in depressed older adults treated with venlafaxine. A secondary objectivewas to analyze 17 other variants in serotonergic system genes (HTR1A, HTR2A, HTR1B, HTR2C, TPH1, TPH2) potentially involved in the mechanism of action of venlafaxine.

The sample included 350 adults age 60 or older with depression, and received open-label venlafaxine. Marshe et al. found that NET variant rs2242446 (T-182C) was significantly associated with remission (odds ratio=1.66, 95% CI=1.13, 2.42, Marshe et al., 2017). Individuals with the rs2242446 C/C genotype were more likely to remit (73.1%) than those with either the C/T (51.8%) or the T/T genotype (47.3%). Individuals with the C/C genotype also had a shorter time to remission than those with the C/T or T/T genotypes and had a greater percentage change in MADRS score from baseline to end of treatment (up to week 12).
A Genome-Wide Approach
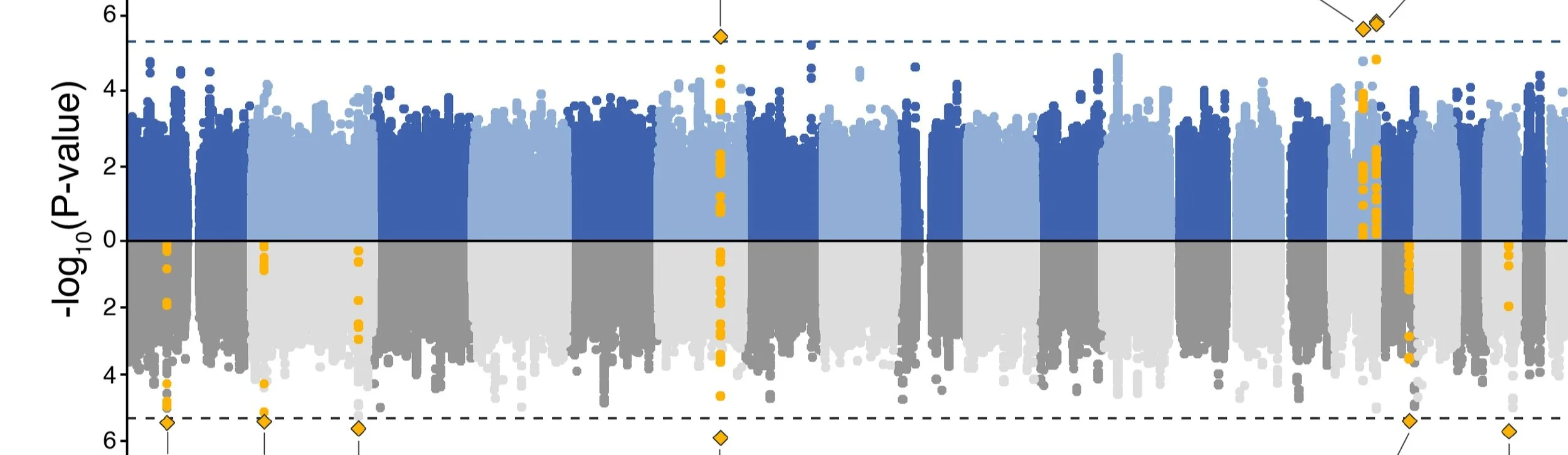
Antidepressant outcomes in older adults with depression are poor, possibly because of comorbidities such as cerebrovascular disease. Therefore, we leveraged multiple genome-wide approaches to understand the genetic architecture of antidepressant response. We conducted a standard genome-wide association study (GWAS) for post-treatment remission status, followed by in silico biological characterization of associated genes, as well as polygenic risk scoring for depression, neurodegenerative, and cerebrovascular disease.

The top-associated variants for remission status and percentage symptom improvement were located in the PIEZO1 gene and an intergenic locus on chromosome 6. Pathway analysis revealed significant contributions from genes involved in the ubiquitin-proteasome system, which regulates intracellular protein degradation with has implications for inflammation, as well as atherosclerotic cardiovascular disease. Although our findings did not reach genome-wide significance, they point to previously-implicated mechanisms and provide support for the roles of vascular and inflammatory pathways in LLD.
Given the polygenicity of complex outcomes such as antidepressant response, we also explored 11 polygenic risk scores associated with risk for Alzheimer's disease and stroke. Of the 11 scores, risk for cardioembolic stroke was the second-best predictor of non-remission, after being male (Accuracy=0.70 [0.59, 0.79], Sensitivity=0.72, Specificity=0.67; p<0.05).

Recent studies highlighted significant associations between treatment-resistant depression (TRD) and PRS for attention deficit hyperactivity disorder (ADHD) in adults as well as a negative association between antidepressant symptom improvement with both schizophrenia and bipolar. Here, Elsheikh et al. sought to validate these findings with symptom remission in the same sample analyzed above (Elsheikh et al. 2024).
We found a nominal (i.e., p value ≤ 0.05) association between symptom remission and both PRS for ADHD and (OR = 1.36 [1.07, 1.73], p = 0.011) and PRS for bipolar disorder (OR = 0.75 [0.58, 0.97], p = 0.031), as well as between percentage symptom improvement and PRS for general intelligence (beta = 6.81 (SE = 3.122), p = 0.03). However, the ADHD association was in the opposite direction as expected, and both associations did not survive multiple testing corrections.
Selected Publications
Elsheikh SSM, Marshe VS, Men X, Islam F, Gonçalves VF, Paré G, Felsky D, Kennedy JL, Mulsant BH, Reynolds CF 3rd, Lenze EJ, Müller DJ. Pharmacogenomics J. 2024 Nov 22;24(6):38.
Pharmacogenetic Implications for Antidepressant Pharmacotherapy in Late-Life Depression: A Systematic Review of the Literature for Response, Pharmacokinetics and Adverse Drug Reactions.
Marshe VS, Islam F, Maciukiewicz M, Bousman C, Eyre HA, Lavretsky H, Mulsant BH, Reynolds CF 3rd, Lenze EJ, Müller DJ. Am J Geriatr Psychiatry. 2020 Jun;28(6):609-629.
Validation study of microRNAs previously associated with antidepressant response in older adults treated for late-life depression with venlafaxine.
Marshe VS, Islam F, Maciukiewicz M, Fiori LM, Yerko V, Yang J, Turecki G, Foster JA, Kennedy SH, Blumberger DM, Karp JF, Kennedy JL, Mulsant BH, Reynolds CF 3rd, Lenze EJ, Müller DJ. Prog Neuropsychopharmacol Biol Psychiatry. 2020 Jun 8;100:109867.
Norepinephrine Transporter Gene Variants and Remission From Depression With Venlafaxine Treatment in Older Adults.
Marshe VS, Maciukiewicz M, Rej S, Tiwari AK, Sibille E, Blumberger DM, Karp JF, Lenze EJ, Reynolds CF 3rd, Kennedy JL, Mulsant BH, Müller DJ. Am J Psychiatry. 2017 May 1;174(5):468-475.